


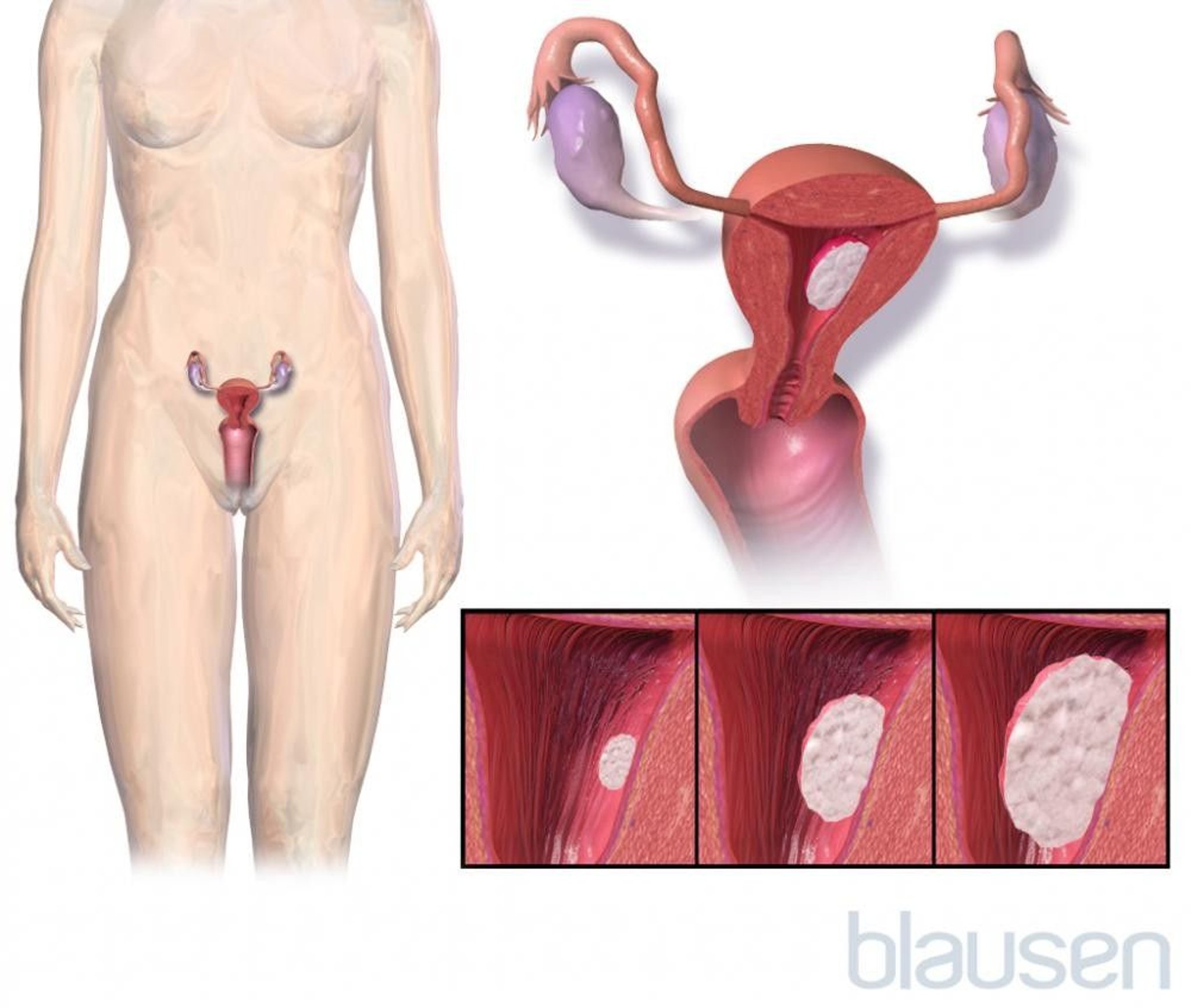
The most common type of cancer of the uterus develops in the lining of the uterus (endometrium) and is called endometrial cancer.
Endometrial cancer usually affects women after menopause.
It typically causes abnormal vaginal bleeding.
To diagnose this cancer, doctors remove a sample of tissue from the endometrium to be analyzed (biopsy).
Treatment usually involves removing the uterus, ovaries, and fallopian tubes and sometimes involves removing nearby lymph nodes, often followed by radiation therapy and sometimes by chemotherapy or hormone therapy.
(See also Overview of Female Reproductive System Cancers.)
Most cancers of the uterus begin in the lining of the uterus (endometrium) and are called endometrial cancer (endometrial carcinoma). Approximately 75 to 80% of endometrial cancers are adenocarcinomas, which develop from gland cells. Sarcomas, another type of cancer, develop from muscle or connective tissue. Sarcomas tend to be more aggressive than other types. Fewer than 5% of cancers in the uterus are sarcomas.
Endometrial cancer is more common in high-resource countries where obesity rates are high. In the United States, this cancer is the 4th most common cancer among women. The American Cancer Society estimates that in 2023, approximately 66,200 new cases of endometrial cancer will be diagnosed and that approximately 13,030 women will die of this cancer. Approximately 80% of these new cases will be early stage with good prognosis, and the remaining 20% will have high-grade or advanced-stage disease.
In the United States, endometrial cancer rates are higher than average in Black, American Indian, and Alaska Native women. Mortality is highest in Black women.
Endometrial cancer usually develops after menopause, most often in women aged 55 to 64 years.

Endometrial cancer is classified as follows:
Type I cancers are more common, respond to estrogen, and are not very aggressive. They tend to occur in younger women, women with obesity, or women going through perimenopause (the years just before and the year after the last menstrual period). The prognosis for women with type I cancers is good.
Type II cancers are more aggressive and tend to occur in older women. Approximately 10% of endometrial cancers are type II. The prognosis for women with type II cancers is poor.
Causes of Uterine Cancer
Endometrial cancer is more common in high-resource countries where obesity rates are high.
Risk factors for endometrial cancer are
Conditions that result in a high level of estrogen and a low level of progesterone
Age over 45
Obesity
A hereditary syndrome called Lynch syndrome (people with this syndrome have a high risk of developing colon and other cancers)
Radiation therapy of the pelvis (which contains the internal reproductive organs, bladder, and rectum)
Conditions that result in a high level of estrogen and a low level of progesterone include the following:
Obesity
Polycystic ovary syndrome or other menstrual problems related to release of the egg (ovulation), because the menstrual cycle can be prolonged during the phase where estrogen is high
Early start of menstrual periods (menarche), late menopause, or both
Never being pregnant (nulliparity)
Estrogen therapy (as a prescription or in herbal products) without a progestin (a synthetic medication similar to the hormone progesterone) taken after menopause
Estrogen-producing tumor
Estrogen promotes the growth of tissue and rapid cell division in the lining of the uterus (endometrium). Progesterone (or progestin medications) causes thinning of the endometrium, which balances the effects of estrogen. Levels of estrogen are high during part of the menstrual cycle. Thus, having more menstrual periods during a lifetime may increase the risk of endometrial cancer. Taking oral contraceptives that contain both estrogen and a progestin appears to reduce the risk of endometrial cancer.
Medications or herbal products that contain estrogen or substances similar to estrogen can cause endometrial cancer if they are not taken with a progestin.
estrogen in the breast, but it has the same effects as estrogen in the uterus. People with breast cancer are not usually given progestins (to balance the effects of estrogen
In approximately 5% of women with endometrial cancer, heredity plays a role. About half of endometrial cancers that involve heredity occur in women who have a hereditary syndrome called Lynch syndrome. People with this syndrome have a high risk of developing colon and other cancers.
Symptoms of Uterine Cancer
Abnormal vaginal bleeding is the most common early symptom of endometrial cancer. Abnormal bleeding includes
Bleeding after menopause
Bleeding between menstrual periods
Periods that are irregular, heavy, or longer than normal
Approximately 6 to 19% of women with vaginal bleeding after menopause has endometrial cancer. Postmenopausal women who have vaginal bleeding should see a doctor promptly, even if there only a small amount of blood or pink, red, or brown staining.
Women with sarcoma usually have abnormal vaginal bleeding. Less commonly, sarcomas cause pain or pressure in the pelvis or abdomen.
Diagnosis of Uterine Cancer
Biopsy
Sometimes dilation and curettage with hysteroscopy
Doctors may suspect endometrial cancer if one of the following is present:
Women have typical symptoms, such as vaginal bleeding after menopause or between periods or irregular, heavy, or unusually long periods.
A Papanicolaou (Pap) test detects cells from the uterus.
If cancer is suspected, doctors take a sample of tissue from the endometrium (endometrial biopsy) and send it to a laboratory for analysis. An endometrial biopsy accurately detects endometrial cancer more than 90% of the time. Alternatively, an ultrasound device may be inserted through the vagina into the uterus (called transvaginal ultrasonography) to evaluate abnormalities. However, a biopsy is still necessary to make the final diagnosis.
If the diagnosis is still uncertain or suggests cancer, doctors scrape tissue from the uterine lining for analysis—a procedure called dilation and curettage (D and C). At the same time, doctors usually view the interior of the uterus using a thin, flexible viewing tube inserted through the vagina and cervix into the uterus in a procedure called hysteroscopy.
If endometrial cancer is diagnosed, some or all of the following procedures may be done to determine whether it has spread:
Blood tests
Kidney and liver function tests (using samples of blood or urine)
Possibly a chest x-ray
If results of the physical examination or other tests suggest that the cancer has spread beyond the uterus, computed tomography (CT) or magnetic resonance imaging (MRI) is done.
Staging of endometrial cancer
Staging is based on information obtained from these procedures and during surgery to remove the cancer.
Stages are based on how far the cancer has spread and the specific type of endometrial cancer (there are different types, some of which are more likely to spread). Stages range from I (the earliest) to IV (advanced):
Stage I: The cancer occurs only in the body of the uterus but not in the lower part (cervix), with possible spread to an ovary for some types of endometrial cancer.
Stage II: The cancer has spread into the muscle layer of the uterus or to the cervix.
Stage III: The cancer has spread to nearby tissues, the vagina, or lymph nodes.
Stage IV: The cancer has spread to the bladder and/or intestines or to distant organs.
Treatment of Uterine Cancer
Surgery to remove the uterus, fallopian tubes, and ovaries
Removal of nearby lymph nodes
For more advanced cancer, radiation therapy with or without chemotherapy
Hysterectomy (surgical removal of the uterus) is the mainstay of treatment for women who have endometrial cancer.
Doctors can remove the uterus, fallopian tubes, and ovaries using one of the following methods:
Making an incision in the abdomen (open surgery)
Using a thin viewing tube (laparoscope) inserted through a small incision just below the navel, then threading instruments through the laparoscope, sometimes with robotic assistance (laparoscopic surgery)
Removing the tissues through the vagina (vaginal surgery)
These methods usually take about 1 to 2 hours and require a general anesthetic. Afterward, vaginal bleeding and pain may occur. Recovery may take up to 6 weeks.
For laparoscopic surgery, thin instruments and a small video camera are inserted through tiny incisions near the navel. The camera sends an image of the abdomen's interior to a monitor. While looking at the monitor, surgeons hold the instruments in their hands and use them to cut and sew tissue.
For robotic-assisted laparoscopic surgery, laparoscopy is done in the usual way. But robotic arms, rather than surgeons, hold the instruments. Surgeons use hand controls to manipulate the arms of the robot. The camera used provides a 3-dimensional, highly detailed (high-definition) image of the interior that is displayed on a console. Surgeons sit at the console to view this image and use a computer that translates their hand movements into precise movements of the instruments.
After laparoscopic or vaginal surgery, hospital stays are shorter than after open surgery (which involves a larger incision). Also, women usually have less pain and fewer complications and can return more quickly to normal activities.
For uterine cancer, total hysterectomy is usually done (the entire uterus including the cervix is removed).
For uterine cancer, nearby lymph nodes are usually removed at the same time as hysterectomy. These tissues are examined by a pathologist to determine whether the cancer has spread and, if so, how far it has spread. With this information, doctors can determine whether additional treatment (chemotherapy, radiation therapy, or a progestin) is needed after surgery.
When the cancer appears to be only in the uterus, doctors may do sentinel lymph node dissection instead of removing all the lymph nodes. A sentinel lymph node is the first lymph node that cancer cells are likely to spread to. There may be more than one sentinel lymph node. These nodes are called sentinel lymph nodes because they are the first to warn that cancer has spread.
A sentinel lymph node dissection involves
Identifying the sentinel lymph node (called mapping)
Removing it
Examining it to determine whether cancer cells are present
To identify sentinel lymph nodes, doctors inject a blue or green dye and/or a radioactive substance, usually into the cervix. These substances travel to the lymph nodes near the uterus and map the pathway from the uterus to the lymph node (or nodes) nearest the uterus. During surgery, doctors check for lymph nodes that look blue or green or that give off a radioactive signal (detected by a handheld device). Doctors remove this node (or nodes) and send it to a laboratory to be checked for cancer. If the sentinel lymph node or nodes do not contain cancer cells, no other lymph nodes are removed (unless they look abnormal).
Treatment of endometrial cancer that has not spread outside the uterus
If the cancer has not spread beyond the uterus, hysterectomy plus removal of the fallopian tubes and ovaries (salpingo-oophorectomy) usually cures the cancer.
Treatment of endometrial cancer that has spread to the cervix or to nearby tissues, the vagina, or lymph nodes
If cancer has spread to the cervix (stage II) or to nearby tissues, the vagina, or lymph nodes (stage III), radiation therapy, sometimes with chemotherapy, is required. Surgery to remove the uterus, fallopian tubes, and ovaries is usually also done.
Treatment of very advanced or recurrent endometrial cancer
Radiation therapy may be given after surgery in case some undetected cancer cells remain. If the cancer has spread to the cervix or beyond the uterus, radiation therapy is usually recommended after surgery. In some cases (as when cancer has spread to the cervix, an ovary, or lymph nodes), surgery plus radiation therapy results in a better prognosis.
If the cancer has spread to distant organs or recurs, chemotherapy, or sometimes immunotherapy, may be used instead of or sometimes with radiation therapy. These medications reduce the cancer’s size and control its spread in more than half of women treated.
Treatment of sarcoma of the uterus
For sarcoma of the uterus (a more aggressive form of endometrial cancer), treatment is hysterectomy plus removal of the fallopian tubes and ovaries (salpingo-oophorectomy) and usually chemotherapy.
If surgery is not possible, radiation and/or chemotherapy is used.
Fertility and menopause after endometrial cancer
Treatment with hysterectomy, chemotherapy, and/or radiation therapy usually makes it impossible for women to become pregnant or to carry a pregnancy to term. However, if being able to have children is important to them, women should talk to their doctor and get as much information as possible about how treatment affects fertility and whether they are eligible for treatments that do not make future pregnancy impossible.
If endometrial cancer is in a very early stage, fertility preservation treatment can sometimes be used. Magnetic resonance imaging (MRI) is done to determine whether the tumor has spread, and a fertility specialist is consulted.
Fertility preservation treatments include
Use of a progestin (a synthetic medication similar to the hormone progesterone) to shrink the tumor instead of a hysterectomy
Sometimes hysterectomy without removing the ovaries
Progestin can be taken by mouth or be given through an intrauterine device
When a hysterectomy is done, menstruation stops because the uterus has been removed. However, if the ovaries are not removed and women are premenopausal, a hysterectomy does not cause menopause because the ovaries continue to produce hormones. Also, when the ovaries are not removed, a woman can use her eggs (and advanced fertility treatments, including having someone else carry the pregnancy) to have children.
When ovaries are removed, menopausal symptoms such as hot flashes and vaginal dryness may occur. If they become bothersome, hormones such as estrogen, a progestin, or both may relieve them.
Prognosis for Uterine Cancer
Prognosis depends on the stage of the endometrial cancer.
Overall, 63% of women are cancer-free 5 years after treatment.
Generally, the prognosis is better if
Endometrial cancer has not spread beyond the uterus.
The cancer is a type that grows relatively slowly.
Women are younger when the cancer is detected.
Prognosis is generally worse with sarcomas than with endometrial carcinoma. Sarcomas develop from muscle or connective tissue. Endometrial carcinoma begin in the lining of the uterus.
Prevention of Uterine Cancer
No measure can prevent endometrial cancer from developing. However, the risk of getting endometrial cancer can be decreased by minimizing or avoiding conditions and activities thought to increase the risk. For example, obesity increases the risk of endometrial cancer. Thus, losing weight, exercising regularly, and eating a healthful diet may be helpful. Also, medications or herbal products that contain estrogen should not be taken alone. They should be taken with a progestin.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
National Cancer Institute: Uterine Cancer: This web site provides links to general information about uterine cancer, as well as links to information about causes, prevention, screening, treatment, and research and about coping with cancer.






